By Katja Grace, 2 February 2015
Penicillin was a hugely important discovery. But was it a discontinuity in the normal progression of research, or just an excellent discovery which followed a slightly less excellent discovery, and so on?
There are several senses in which penicillin might have represented a discontinuity. Perhaps its discovery was a huge leap in effectiveness, saving lives at a rate nobody thought possible. Or it might have been dramatically cheaper than expected. Or it could have heralded a step up in life expectancy, or a step down in disease prevalence.
We investigated this, to add to our list of cases of discontinuous technological progress, or alternatively to our new list of things we have investigated to potentially add to that list, but didn’t.
To make life easier, we focused on penicillin as used to remedy syphilis in particular. Our only conscious reason for choosing syphilis was that penicillin is used to cure it. It is also a disease against which penicillin was considered an important step forward.
First, was penicillin a huge step forward in effectiveness, compared to the usual progress? In the field of syphilis prevention, the recent competition was actually tough. A treatment for syphilis developed thirty years earlier was literally nicknamed ‘magic bullet’ and spawned a nobel prize as well as a frightening looking movie. More quantitatively, existing treatments at the time of penicillin’s introduction in the early 40s were apparently ‘successful’ for about 90% of patients who took them, and it doesn’t look like penicillin did better initially. So probably penicillin didn’t jump ahead on effectiveness.
However a big difference appears to be hidden within ‘patients who took them’. The ‘magic bullet’ was an arsenic compound, unstable in air, needing frequent injections for weeks, and producing risk to life and limb. According to the only paper I found with figures on this, about three quarter of patients ‘defected’ before receiving a ‘minimum curative dose’ of an arsenic and bismuth treatment, which suggests that while earlier cures were not obviously worse than dying of syphilis, they were also not obviously better (or else perhaps people dropped out when the severity of their side effects prohibited them from continuing). Penicillin allowed virtually everyone to get a minimum curative dose. So it’s possible that penicillin represented a discontinuity in this more inclusive success measure, but alas we don’t have the data to check. If penicillin really treated four times as many patients as recent precursors, and both cured most of them, and many would die otherwise, and little progress had happened on this measure since salvarsan, then penicillin would be worth at least thirty years of progress, and perhaps much more.
(I hear you wondering, if this magic bullet was so much better than its precursors, what on earth were the precursors? Breathing mercury was one. From before the 16th century until the discovery of salvarsan, ‘mercury treatments’ were common. Early mercury treatments included rubbing mercury into one’s body, and inhaling the mercury fumes, while later ones involved more sophisticated injections of mercury compounds).
I should point out that I’m confused by these apparently high defection rates. Syphilis has an untreated mortality rate of 8-58%, so defection from treatment would appear to be living pretty dangerously. This suggests I’m wrong about something, just so you know. Nonetheless, being right about everything doesn’t seem cost-effective here.
So far it seems like penicillin’s main advantage was in being less costly (including costs such as suffering and complications). Was this an abrupt change? It is hard to get figures for the inclusive costs of penicillin and its precursors, let alone a longer term trend to compare to. We can say that penicillin took around eight days at the very start, while other treatments took more than twenty. And penicillin seems to have been a lot less dangerous. However qualitatively speaking, salvarsan also sounds a lot less dangerous than mercury treatments. There were also further improvements in safety prior to penicillin, such as in neosalvarsan. So guessing qualitatively, penicillin might have been a few decades worth of previous progress in reducing costs, but probably not much more.
Even at the height of syphilis, the disease was not common enough that resolving all of it in one year would produce a visible change to life expectancy, so we shan’t look at that.
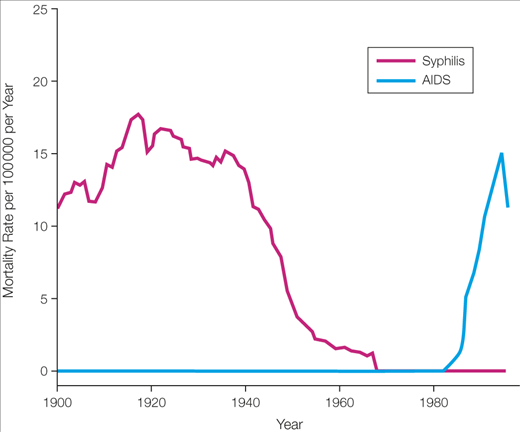
Did syphilis rates decline abruptly? Both having syphilis and dying from it became much less common during the 1940s, which is probably due in large part to antibiotics (see figures 1 and 2). Deaths from syphilis declined by 98%. However, as you can see, these were not abrupt changes. Things got modestly better every year for decades.

In sum, it seems unlikely that there was abrupt progress on drug effectiveness conditional on completing the treatment, or on how many people had or died from syphilis. There may have been abrupt progress in overall costs or in drug effectiveness conditional on being offered the treatment, but these have been too hard to evaluate here.
So for now, we add it to the list of things we checked, but not the list of things that were abrupt. The list of things we checked is part of a larger page about this project, in case you are curious. We also looked into the Haber process recently, but didn’t think it involved much discontinuity. We might blog about it at some point.
Some other interesting facts about syphilis and penicillin I learned:
- A pre-penicillin treatment for neurosyphilis was to give the patient malaria, because malaria mitigated the syphilis, and was considered more treatable than syphilis.
- Early on, penicillin was so valuable that doctors recycled what hadn’t been metabolized by extracting it from patients’ urine.
- There is a whole wikipedia page of previous occasions in history where people observed that mould prevented bacterial infection, more or less, but apparently didn’t follow up that much.


{kind=link}
I find this article etmrexely interesting. It doesn’t shock me even slightly that Facebook users have a higher rate of syphilis, however the way it is phrased seems a little off. The way it is put makes it seem like if you use Facebook, you are more likely to contract syphilis. However, I feel that Facebook users are already more vulnerable to contracting the disease, as that is who they are. Facebook users are by default already much more social than non-Facebook users, so their willingingness and probability to contract a disease from a social scene is higher than those who do not socially network. I feel, in this case, that Facebook, as well as many other social media networking sites, act as enablers more than anything. We are the actors and the ones who, due to our social habits, will go out and contract whatever we choose. Facebook just may be the channel we chose to do it through.
If you’re looking to buy these articles make it way easier.
Hi thanks for the information
I would like to invite you all to visit our clinic for more info about
how to treat your viruses. Please click the link below to reach us!
Thank you for all your support and may we help you too with your problem.
Good day and God Bless!
Thank you by syphilis prevention